

Comprehensive Pharmacy Services customizes and implements hospital medication reconciliation program to drive transitions of care performance.
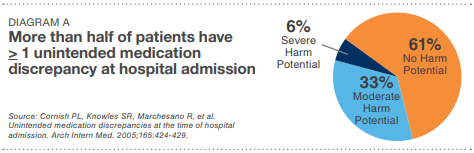
Patients often receive new medications or have changes made to their existing medications at times of transitions in care—upon hospital admission, transfer from one unit to another during hospitalization, or discharge from hospital to home or another facility. Caregivers at these transition points may inadvertently omit needed medications, unnecessarily duplicate existing therapies, or contain incorrect dosages. These discrepancies place patients at risk for adverse drug events, which have been shown to be one of the most common types of adverse events after hospital discharge and a key driver of hospital readmissions (see Diagram A).(1)
Medication reconciliation refers to the process of avoiding such inadvertent inconsistencies across transitions of care by reviewing the patient’s complete medication regimen at the time of admission, transfer, and discharge and comparing it with the regimen being considered for the new setting of care.
Hospitals will lose a combined total of $420 million in reimbursements, penalized for failing to meet readmissions targets set by the Centers for Medicare and Medicaid Services (CMS). According to CMS, the average readmissions rate was 18.4 percent in 2012(2).
There’s a reason for the readmission problem. Studies show that patients are often discharged from the hospital confused and don’t know how to take their prescriptions properly(3), and what’s worse, patients may duplicate, miss or take the wrong prescriptions that are not in the care plan.(4)
With maximum CMS penalties set at 3%, the financial consequences of failing to meet CMS targets for readmissions are very real. Statistics paint a bleak picture of the challenges confronting hospitals as they work to stem the tide of preventable readmissions:
• 20% of Medicare patients will be readmitted to the hospital within 30 days of discharge(5)
• 66% of emergency readmissions for patients over 65 years old are due to adverse medication events(6)
• 19% of Medicare discharges are followed by an adverse medical event within 30 days, and 2/3 of these are preventable(7)
• 20% of patients do not fill their prescriptions(8)
All of these dynamics led to the pilot program outlined in this case study, where the leading community hospital sought to leverage pharmacy resources to build a medication reconciliation program during transitions of care, from hospital admissions to postdischarge to the patient’s home. The hospital wanted to manage the high risk and complex medication regimens, patient specific risk factors, comorbidities and adverse drug events associated with an increased rate of readmissions.
Medication Reconciliation During Transitions of Care: Pilot Goals
• Reduce medication issues that could lead to readmissions
• Improve patient outcomes by enhancing communication related to medications, pre- and post-discharge
• Target Core Measure conditions for readmission scores, including congestive heart failure, chronic obstructive pulmonary disease, pneumonia and myocardial infarction patients discharged to home
• Reduce CMS and commercial payer reimbursement penalties related to readmissions
A study performed by the University of California found that engaging patients with credible information delivered by a pharmacist yields results, including reduced medication-related ER visits and unnecessary readmissions(9).
That was the premise for piloting a medication management program customized to JFK Medical Center’s needs. The CPS telepharmacy team had access to the hospital’s EHR, the ability to document patient interactions within the hospital’s system and provide customized reporting to the primary care physician or case manager.
We chose to target the JFK Medical Center’s Core Measure patient population units including congestive heart failure, pneumonia, COPD, and myocardial infarction, driven by a three-part program:
Medication Reconciliation
• We built an admission and discharge medication reconciliation process that delivered a more complete picture of inpatient, outpatient and retail prescription history, which enabled more accurate reconciliation, variance identification and reporting.
• We used a proprietary medication reconciliation process; including access to a national pharmacy claims database as well as medication lists and medical chart information from the hospital’s electronic health record to identify and correct variances.
• CPS pharmacists made evidence-based disease state intervention recommendations to the hospital care team for therapy optimization and greater patient safety.
• Discharge medication education is provided by a licensed pharmacist, not a nurse or pharmacy technician
Post-Discharge Support
• Pharmacist review of discharge medication orders
• 48 hours post discharge patient support includes phone conversation with patient to assess filling of discharge meds and understanding of medication therapies, as well as identification of significant clinical issues that might lead to readmission
• 24/7 access to a clinical pharmacist via phone or multi-media communications
• Scheduling calls to patient’s home
• Information gathered from patient coaching is submitted to hospital pharmacists, nurses, and physicians
Our program for medication reconciliation during transitions of care caught medication errors, improved patient safety and reduced readmissions across a number of the Core Measure units:
• 44% of the targeted patients are discharged to home in our case study.
• 85% of patients, discharged to home, received pre-discharge medication counseling by a pharmacist.
• 82% of patients, discharged to home, were successfully contacted post discharge by a pharmacist.
• 13% of patients, during the post discharge follow up call, could not validate the filling of their discharge prescriptions.
• 11% of patients, during the post discharge follow up call, were identified by the pharmacist as having a significant clinical issue:
- 96% were referred to their primary care physician
- 4% were referred to the emergency room for further care
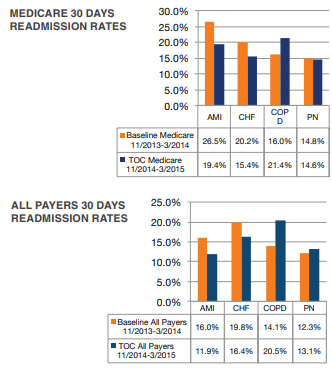
• Readmission rates declined for the AMI/CHF patient populations, COPD rates increased (however, that was driven by an anomaly staff shortage in that particular unit), while pneumonia readmission rates were relatively unchanged.
More broadly outside this case study, CPS has driven successful outcomes across transitions of care programs, which have reduced readmissions by over 30% in certain disease states and increased HCAHPS scores as much as 13%.
Our programs have reduced CMS penalties and unscheduled visits to emergency departments and urgent care, increased early identification of therapy failures post-discharge, enhanced the patient experience, improved clinical outcomes, and lowered total cost of care.

Founded nearly 50 years ago and employing over 2,500 clinical, regulatory, and operational pharmacy professionals, Comprehensive Pharmacy Services is the nation’s oldest and largest provider of pharmacy support services to more than 700 hospitals and healthcare facilities across the United States and Puerto Rico. CPS helps hospital pharmacists tackle complex problems such as medication reconciliation, hyper-inflated drug costs, standardization, centralized distribution, regulatory & compliance, and 340B programs leading to increased quality, reduced admissions and lower costs.
This post is related to:
Adherence, Compliance, Remote Monitoring, Med Sync Medication Inventory Management & Procurement
